General Information
The Modern Treatment of Lithiasis of the Urinary System
In recent decades, an increase in the frequency of uroliths has been observed. Stone formation is a complex process whose pathogenesis is not yet fully understood. The average lifetime risk of developing urolithiasis is 5-10%. The ratio of presenting stones between men and women is approximately 3:1 with an increase in presentation in the 4th and 5th decades of life. The main problem of all types of lithiasis is the recurrence of the disease. Early diagnosis and treatment of the recurrence is a key concern of doctors to avoid possible damage to kidney function.
Based on the chemical composition of the stone and the severity of the disease, there are various categories of patients.
Patients with non-calcareous stones such as inflammatory stones, uric acid, sodium urate and ammonium urate stones and cystine stones.
Patients with calcium stones are divided into those who have a stone for the first time that left no residue, those with stone residue, recurrent stone without residue after treatment, with residue after treatment and with a specific risk factor.
Patients who have special risk factors for the formation of lithiasis need special attention. These are the patients who have an early onset of the disease (younger than 25 years), stones containing brucite and the existence of a functioning kidney. Also patients with hyperparathyroidism, renal tubular acidosis, jejunoileal bypass, Crohn’s disease, enterectomy, malabsorption syndrome and hyperthyroidism.
Patients taking calcium and vitamin D supplements, large doses of ascorbic acid (>4 g/day), sulfonamides, triamterene, and indinavir should also be monitored.
Anatomical abnormalities such as tubular ectasia, pyeloureteric junction stenosis, ureteral stricture, vesicoureteral reflux, horseshoe kidney, and ureterocele can be causes of stone formation.
Diagnostic Imaging and Laboratory Testing
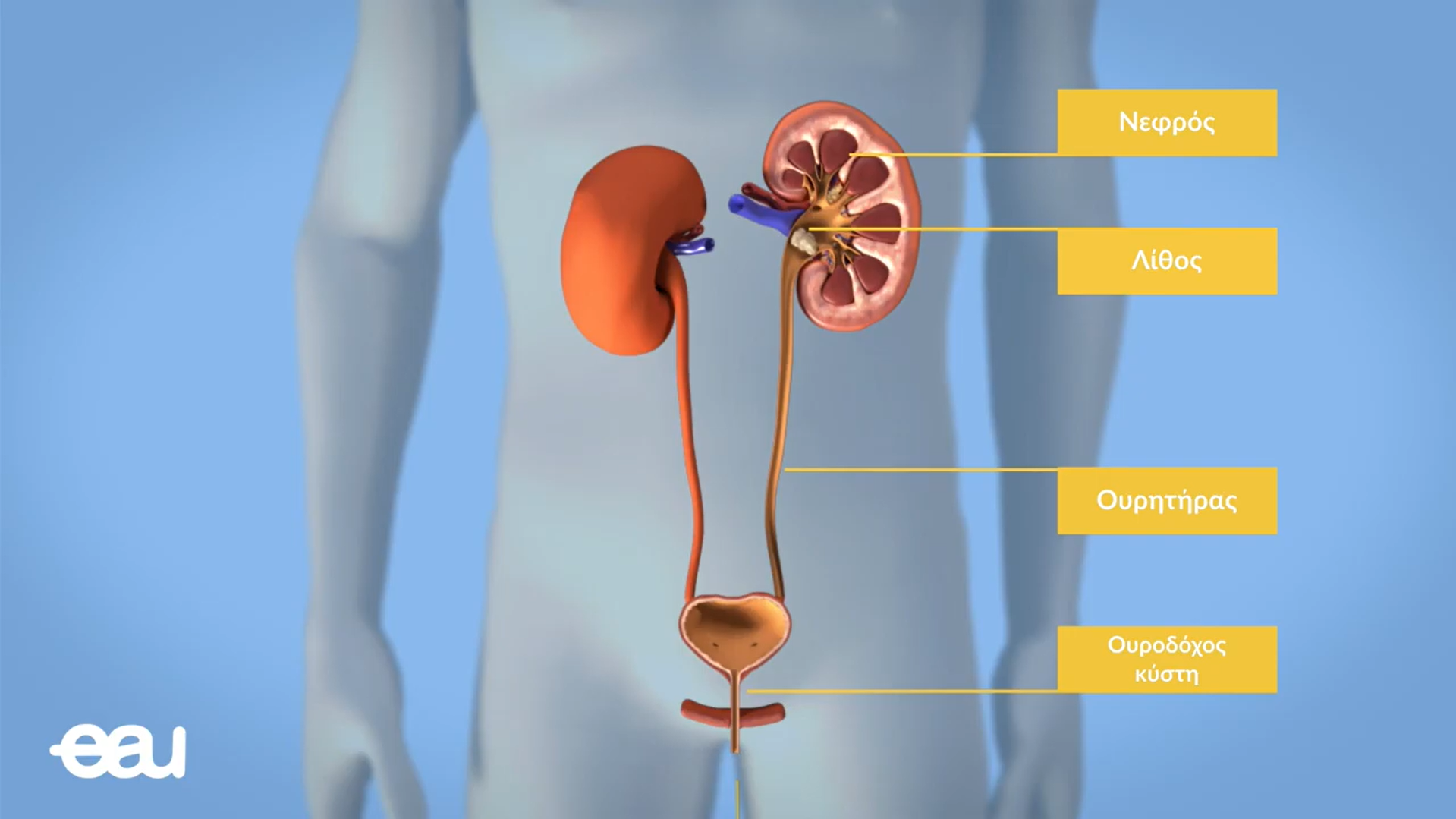
Kidney colic has different symptoms depending on the location of the stone. So the pain spreads from top to bottom. When the stone is in the kidney, the pain remains mainly in the lumbar region. Procystic stones cause a tendency to urinate and pain that reflects on the testicles or, in women, on the labia majora. Οι άρρωστοι έχουν επίσης τάση για εμετό, μετεωρισμό της κοιλιάς και ίσως αντανακλαστικό ειλεό. Η παρουσία πυρετού σημαίνει πολλές φορές επιπλοκή λόγω υδρονέφρωσης και λοίμωξης και απαιτεί άμεση χορήγηση αντιβιοτικών και σε περίπτωση υδρονέφρωσης άμεση παροχέτευση του νεφρού.
Στην διαφορική διάγνωση πρέπει να σκεφτούμε τον κωλικό χοληδόχου, τη σκωληκοειδίτιδα και στις γυναίκες τη συστροφή κύστης της ωοθήκης η την εξωμήτρια κύηση.
Η κλινική διάγνωση πρέπει να στηριχθεί στην κατάλληλη απεικόνιση. Η συνήθης εξέταση περιλαμβάνει απλή ακτινογραφία κοιλιάς και υπερηχογράφημα. Εάν υπάρχει υποψία μη ακτινοσκιερού λίθου γίνεται η ελικοειδής αξονική τομογραφία χωρίς σκιαγραφικό. Η πυελογραφία μας δίνει πληροφορίες για την ακριβή θέση του λίθου και πιθανές ανωμαλίες του ουροποιητικού συστήματος .Σε ειδικές περιπτώσεις μπορεί να είναι αναγκαία η εξέταση με ανιούσα η κατιούσα πυελογραφία.
Ο εργαστηριακός έλεγχος στην οξεία φάση περιλαμβάνει γενική αίματος και ουρών ,με καλλιέργεια σε περίπτωση πυρετού, πηκτικό μηχανισμό και ηλεκτρολύτες.
Σε όλους τους ασθενείς με λιθιασική νόσο πρέπει να γίνεται ανάλυση του λίθου και ανάλογα της σύστασης του περαιτέρω αναλυτικό πρόγραμμα μεταβολικής εκτίμησης.
Indications for Active Stone Removal
The decision to treat the stone depends on its size, location and shape. If the stone is smaller than 4 mm, it is expected to be expelled automatically in 80% of patients. For stones larger than 7 thousand the percentage of automatic expulsion varies between 25% and 70%. The removal consists of stones larger than 6/7mm.
An absolute indication for stone removal is in cases of persistent pain despite medication, obstruction with impairment of renal function, urinary tract infection, risk of pyonephorus or uroseptics, bilateral obstruction and obstructive stone in a single functional kidney.
Principles of Active Stone Removal
With the use of modern methods, the removal of stones of the urinary system through open surgery is the absolute exception and has been necessary in the last 20 years in less than 1% of patients.
The invention in 1980 of extracorporeal lithotripsy (ESWL) by the Urology Clinic of the University of Munich in combination with the use of Percutaneous Nephrolithotripsy and Ureteroscopy revolutionized the treatment of Urolithiasis.
Today it is no longer necessary for the patient to undergo painful open operations with several days of hospitalization, loss of part of the function of the kidney or with the risk of losing the entire kidney for the removal of a stone of any size or location.
This is of particular importance for the treatment of lithiasis in children.
In fact, according to the guidelines of the European Union of Urologists (EAU), the open removal of stones of the urinary system is the absolute last option.
Treatment Methods and Indication
Principles of kidney stone removal
- Stones smaller than 2 cm are best treated with extracorporeal lithotripsy (ESWL) and as a second option with percutaneous lithotripsy (PNL)
- Uric acid stones with ESWL and chemodialysis.
- Stones larger than 2 cm or coralline with percutaneous lithotripsy (PNL) and as a second option initially with extracorporeal lithotripsy (ESWL). A combination of both methods is usually required.
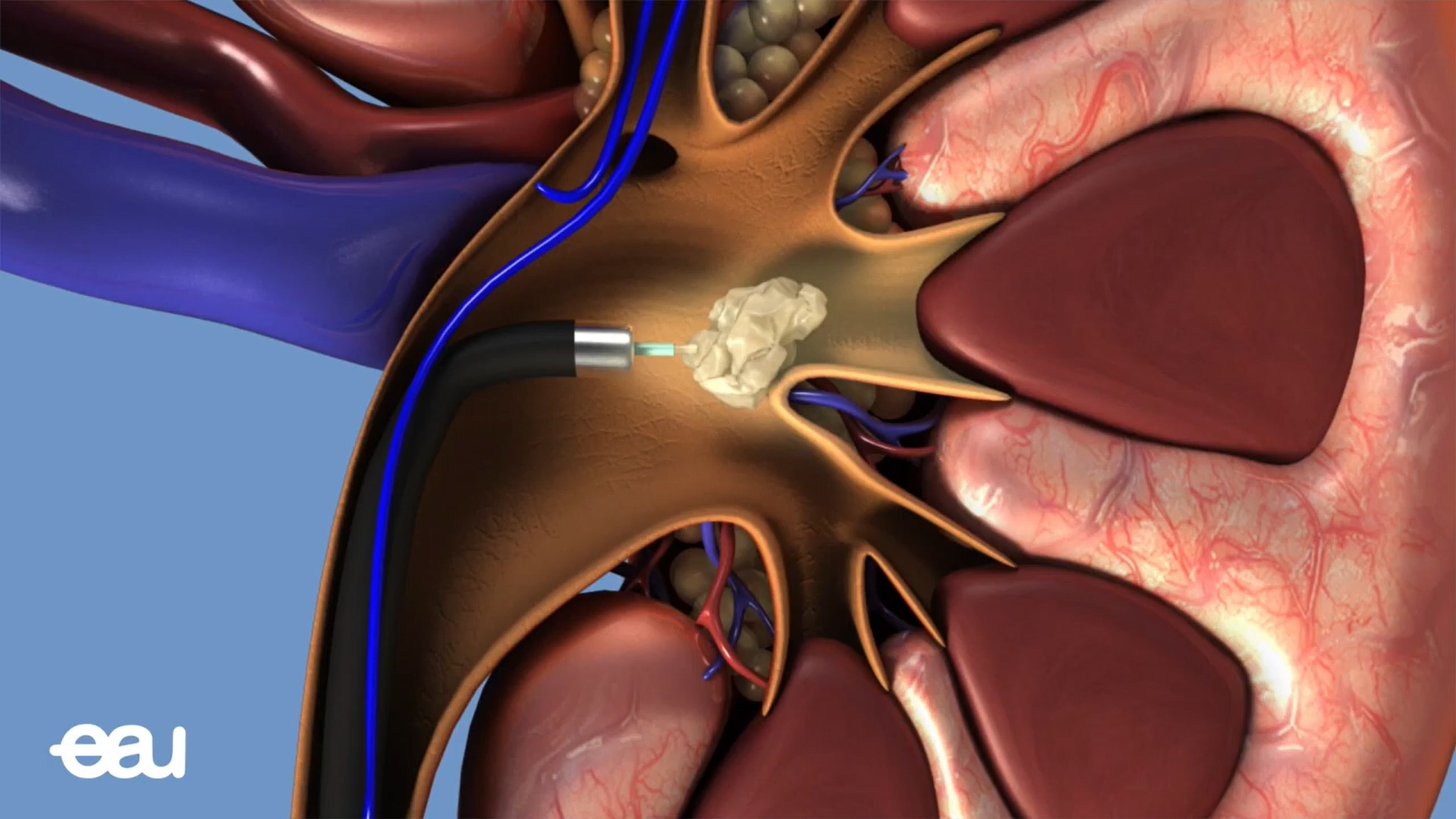
Percutaneous Lithotripsy (PNL)
Play Video about Διαδερμική Λιθοθρυψία
Extracorporeal Lithotripsy (ESWL)
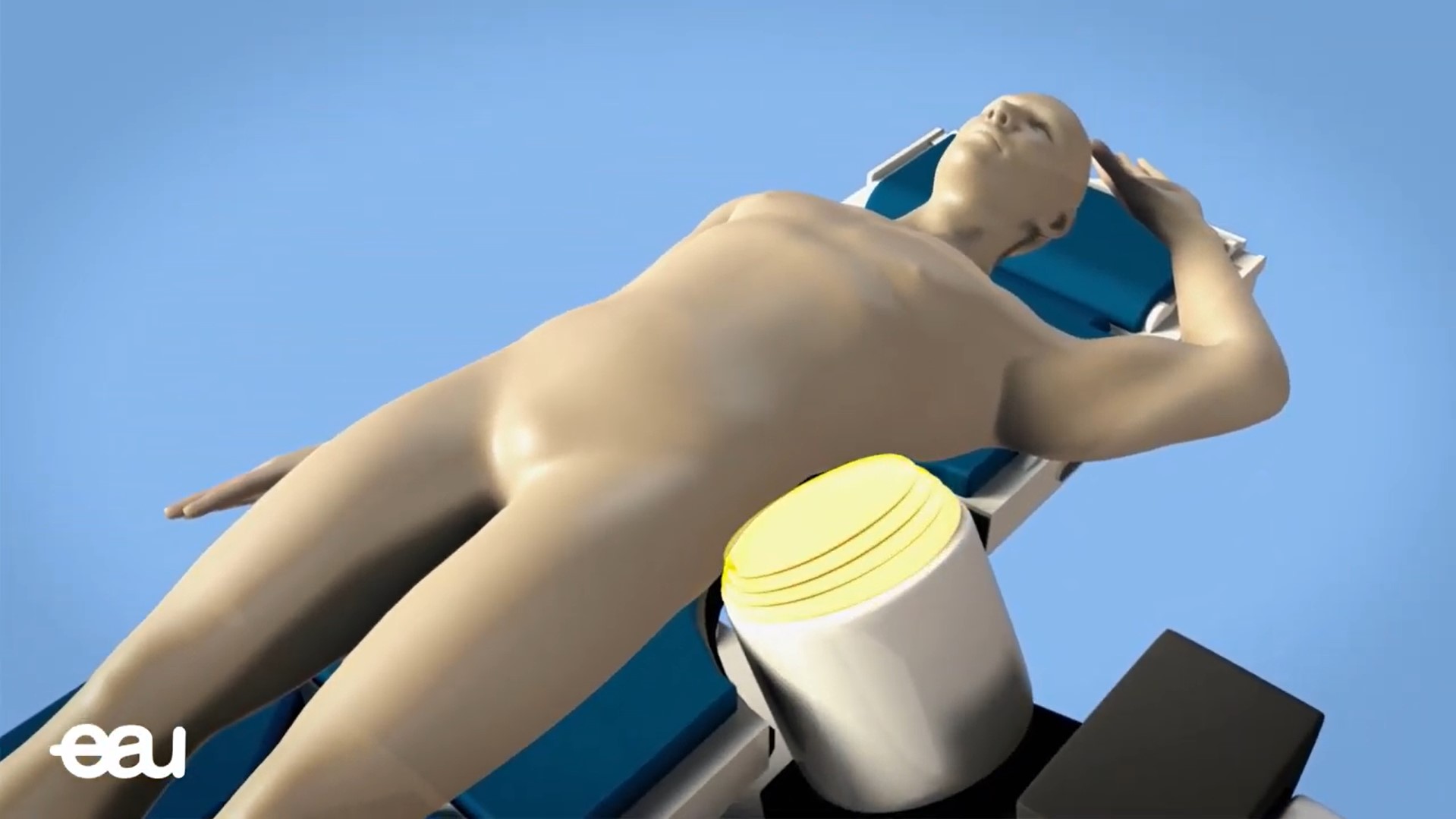
Play Video about Εξωσωματική Λιθοθρυψία
Ureteroscopy
Play Video about Ουρητηρονεφροσκόπηση
Cystoscopy
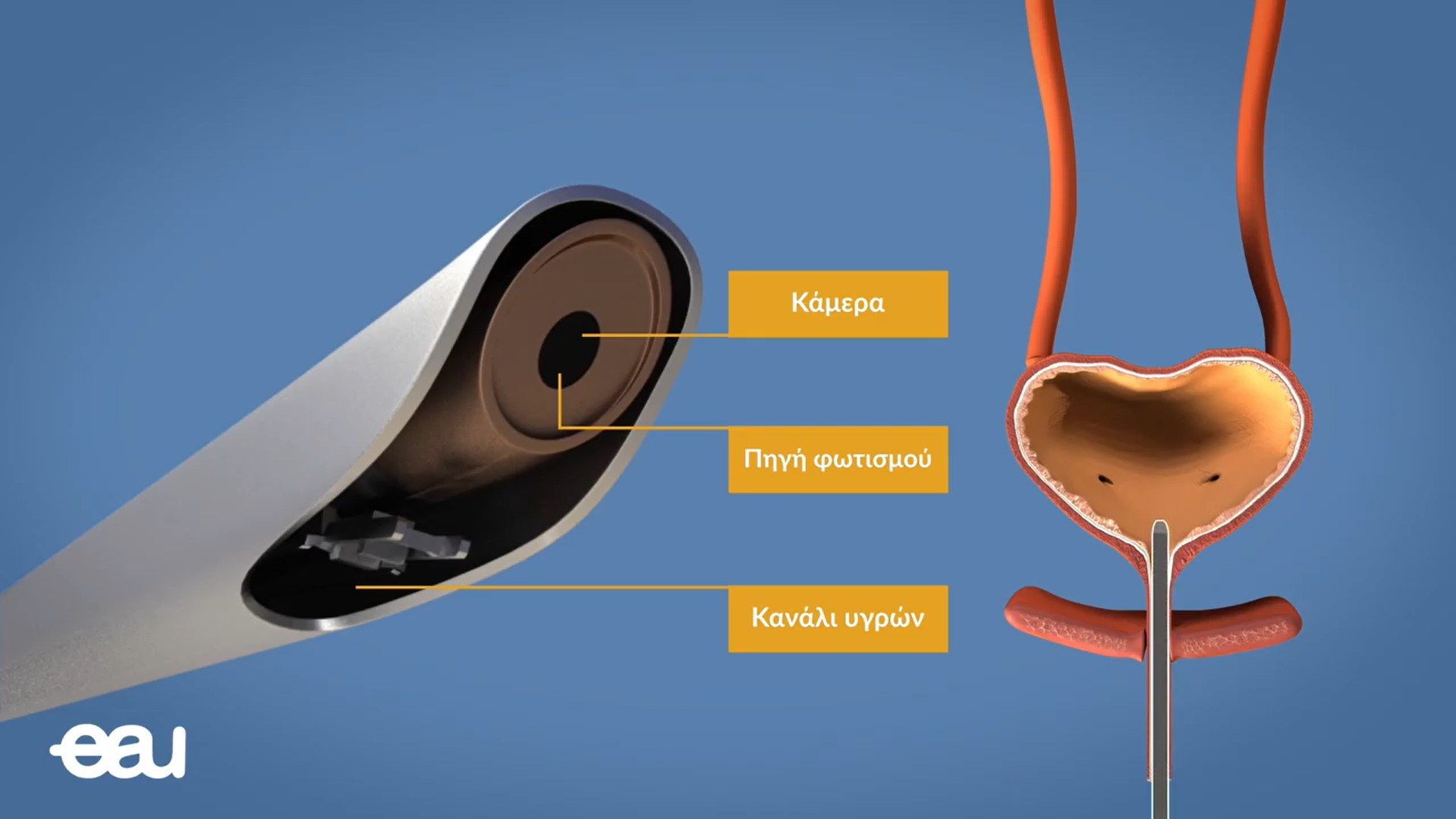
Play Video about Κυστεοσκόπηση